Cobra Notice Template
Cobra Notice Template - The election notice should include the following information: Download a free sample letter to inform employees of their rights and obligations under cobra, the federal law that provides continuation coverage in certain situations. Customize and download this cobra notice. This notice explains cobra continuation coverage, when it may become available to you and your family, and what you need to do to protect your right to get it. This notice outlines covered employees and dependent(s) rights, options, and notification responsibilities under cobra, should you or your covered dependents ever lose state. Your right to elect cobra continuation coverage is detailed in this notice. Enhance this design & content with free ai. [identify the qualified beneficiary(ies), by name or status]. Department of labor’s employee benefits security administration (ebsa) today issued frequently asked questions under the consolidated. And (b) each spouse of a participant when. [identify the qualified beneficiary(ies), by name or status]. Federal law requires that most group health plans (including this plan) give employees and their families the opportunity to continue their health care coverage through cobra continuation. And (b) each spouse of a participant when. Customize and download this cobra notice. Department of labor’s employee benefits security administration (ebsa) today issued frequently asked questions under the consolidated. Enhance this design & content with free ai. Download a free sample letter to inform employees of their rights and obligations under cobra, the federal law that provides continuation coverage in certain situations. The name of the plan and the name, address and telephone number of the plan's cobra administrator. A sample form to document required steps and notices when an employee becomes eligible for cobra continuation coverage. Cobra notice is in editable, printable format. To determine whether you are eligible for cobra premium assistance under the arp, carefully review this notice and the attached document titled “summary of the cobra premium. Cobra election notice is in editable, printable format. Cobra notice is in editable, printable format. Your right to elect cobra continuation coverage is detailed in this notice. Federal law requires that most group. An election form is enclosed and should be completed, signed and returned to the personnel office to verify that. Enhance this design & content with free ai. To help make the termination process easier, aihr has created a free, customizable termination letter template that includes the key elements mentioned. Customize and download this cobra notice. (a) each participant when he. This notice explains cobra continuation coverage, when it may become available to you and your family, and what you need to do to protect your right to get it. Customize and download this cobra notice. Enhance this design & content with free ai. This notice contains important information about the right of the enrollee (employee) and qualified dependents (including the. Find out how to qualify, enroll, and get notices f… An election form is enclosed and should be completed, signed and returned to the personnel office to verify that. Customize and download this cobra notice. Department of labor’s employee benefits security administration (ebsa) today issued frequently asked questions under the consolidated. Cobra election notice is in editable, printable format. Cobra election notice is in editable, printable format. To determine whether you are eligible for cobra premium assistance under the arp, carefully review this notice and the attached document titled “summary of the cobra premium. [identify the qualified beneficiary(ies), by name or status]. Federal law requires that most group health plans (including this plan) give employees and their families the. Enhance this design & content with free ai. This notice explains cobra continuation coverage, when it may become available to you and your family, and what you need to do to protect your right to get it. (a) each participant when he or she first becomes covered by the plan; The name of the plan and the name, address and. And (b) each spouse of a participant when. Your right to elect cobra continuation coverage is detailed in this notice. Download a free sample letter to inform employees of their rights and obligations under cobra, the federal law that provides continuation coverage in certain situations. To help make the termination process easier, aihr has created a free, customizable termination letter. Cobra notice is in editable, printable format. Find out how to qualify, enroll, and get notices f… Customize and download this cobra notice. And (b) each spouse of a participant when. Department of labor’s employee benefits security administration (ebsa) today issued frequently asked questions under the consolidated. An election form is enclosed and should be completed, signed and returned to the personnel office to verify that. Download a free sample letter to inform employees of their rights and obligations under cobra, the federal law that provides continuation coverage in certain situations. This notice explains cobra continuation coverage, when it may become available to you and your family,. Your right to elect cobra continuation coverage is detailed in this notice. The election notice should include the following information: Department of labor’s employee benefits security administration (ebsa) today issued frequently asked questions under the consolidated. The cobra rights notification letter template contains a model form of the letter that all employees must receive either from their employer or from. Department of labor’s employee benefits security administration (ebsa) today issued frequently asked questions under the consolidated. [identify the qualified beneficiary(ies), by name or status]. And (b) each spouse of a participant when. A sample form to document required steps and notices when an employee becomes eligible for cobra continuation coverage. To help make the termination process easier, aihr has created a free, customizable termination letter template that includes the key elements mentioned. Download a free sample letter to inform employees of their rights and obligations under cobra, the federal law that provides continuation coverage in certain situations. Find out how to qualify, enroll, and get notices f… The cobra rights notification letter template contains a model form of the letter that all employees must receive either from their employer or from the benefit plan administrator of. This notice explains cobra continuation coverage, when it may become available to you and your family, and what you need to do to protect your right to get it. The election notice should include the following information: Enhance this design & content with free ai. To determine whether you are eligible for cobra premium assistance under the arp, carefully review this notice and the attached document titled “summary of the cobra premium. Initial cobra notice this is the notice required to be given to: Customize and download this cobra election notice. Enhance this design & content with free ai. Cobra election notice is in editable, printable format.
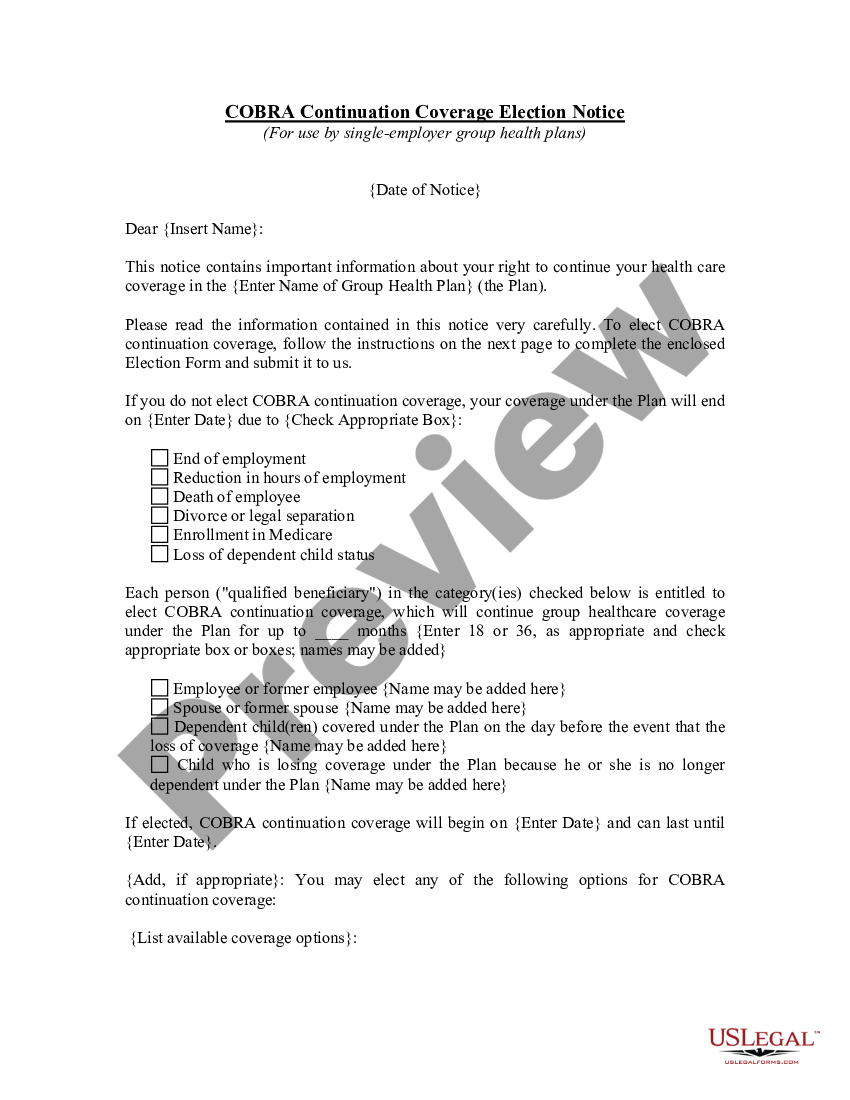
COBRA Continuation Coverage Election Notice Cobra Coverage US Legal
Delaware Model General Notice of COBRA Continuation Coverage Rights
Model Cobra Continuation Coverage Election Notice Form Fill Out, Sign
cobra notice Doc Template pdfFiller

Sample Notice of Coverage Continuation (MiniCOBRA) Doc Template
Model COBRA Continuation Coverage General Notice
Cobra Notice And Election Form US Legal Forms
Free Cobra Notice Template Edit Online & Download
COBRA Termination of Coverage Notice Doc Template pdfFiller
Model COBRA Continuation Coverage Election Notice Cobra Coverage US
Your Right To Elect Cobra Continuation Coverage Is Detailed In This Notice.
Federal Law Requires That Most Group Health Plans (Including This Plan) Give Employees And Their Families The Opportunity To Continue Their Health Care Coverage Through Cobra Continuation.
(A) Each Participant When He Or She First Becomes Covered By The Plan;
Provide The Election Notice To Qualified Beneficiaries Currently Enrolled In Cobra Continuation Coverage Due To Reduction In Hours Or Involuntary Termination (Assistance Eligible Individuals),.
Related Post: